joea73
Views
Online Status OFFLINE
Member Since 4 years ago
Last Online 2 days ago
Last Updated 2 weeks ago
Forum Replies Created
-

joea73
MemberJuly 2, 2024 at 2:12 am in reply to: Metastatic bladder cancer spread to liver and other placesI think it is best to contact your doctor if you are concerned with any side effect of PADCEV.
I do not have any experience with Padcev. But I know some about it and its associated side effects. Pacdev is a targeted chemotherapy. It works differently from Cisplatin systemic chemotherapy and Keytruda systemic PD-1 checkpoint inhibitor based immunotherapy. Padcev belongs to Antibody-Drug Conjugate. It uses synthesized antibodies as delivery vehicles which attach specifically to the cell which expresses Nectin-4 proteins on its cell membrane. Once it reaches the target cell, which are highly expressed on the cell membrane of bladder cancer. Once Padcev reaches the target cell, it releases highly toxin called MMAE into the cell. MMAE, which disrupts microtubule dynamics during cell division cycle, will lead the cell to cell cycle arrest and apoptosis (self programmed death). Bladder cancer cells are known to express Nectin-4 protein on its cell membrane. This is why Padcev works for bladder cancer. Unfortunately, Nectin-4 protein is expressed on healthy cells of tissues of other organs, including for example. skin, digestive system, bone marrow, pancreas etc. Padcev will attack healthy cells of those organs and that is the root cause of side effects.
If cells of bone marrows are attacked, red blood cells and white blood cells which are produced in bone marrows will decrease. Red blood cells carry oxygen. Oxygen and glucose are consumed by mitochondria which generate energy used in our body. This may lead to tiredness. If white blood cells are reduced it weakens the immune system. Perhaps, you can request for a blood test which checks red blood cell / hemoglobin, platelet counts and white blood cell counts.
Fever can be caused by various reasons such as inflammation which are the result of PADCEV treatment.
Below is the list of expected side effects and recommended actions by the Ontario Province Healthcare system in Canada. I have found the list is well explained. What to do with fever is extensively explained.
https://www.cancercareontario.ca/en/drugformulary/drugs/infosheet/73996
Similar information from University of Pittsburgh Cancer Center.
-
joea73
MemberJune 27, 2024 at 7:18 pm in reply to: Re:Metastatic Bladder Cancer, treatment side effects<div>
I have never taken Eradafitnib, so I cannot tell from my experience. But I know someone who have had Erdafitnib.
I am sorry to hear that your husband is experiencing side effects BALVERSA® (erdafitinib). BALVAERSA is a so-called FGFR kinase inhibitor. It is like a switch to start a cell division cycle. FGFR of cancer cells are often defective, so cancer cells are constantly dividing and duplicating more cancer cells. BALVAERSA stops producing more cancer cells by disabling the FGFR switch.
Side effects happen because normal cells of other tissues, especially fast growing tissue such as nails, have many FGFRs because they need to grow faster. It is also known that FGFR have been detected in various cell types within the oral cavity, which I think is the cause of mouth soreness.
</div><div>Pain in the soles seems to be palmar–plantar erythrodysesthesia syndrome (PPES). PPES typically affects the palms of the hands and the soles of the feet, causing a range of symptoms from mild redness and swelling to severe pain and blistering. PPES is also mentioned as side effect of FGFR kinase inhibitor.
</div>In terms of treatment, I think urologist and dermatologist should be consulted. Below are information I have found on internet. The information is only from reputable medical professionals.
Below recommendations are mentioned in a published paper
Dermatologic Adverse Events Associated with Selective Fibroblast Growth Factor Receptor Inhibitors: Overview, Prevention, and Management Guidelines
https://theoncologist.onlinelibrary.wiley.com/doi/full/10.1002/onco.13552
Nail Changes
Counseling and education on the potential for nail changes are essential before initiation of treatment with FGFR inhibitors. Preventive strategies include avoidance of prolonged contact with water, repeated trauma, friction, and pressure on nails and nail beds. The use of protective gloves and limiting use of nail polish removers and nail hardeners is also helpful. Patients are also advised to avoid biting nails or cutting nails too short and to use topical emollients and loose-fitting socks and footwear. Preventive correction of nail curvature may be considered.
PPES
Prevention strategies for PPES include prophylactic removal of hyperkeratotic areas, application of moisturizing cream containing urea ≥10%, pedicures, and cushioning of callused areas using soft or padded shoes [48]. Other preventive tactics include avoidance of activities that cause force or rubbing on the hands and feet during the first 6 weeks of treatment and limiting contact with harsh chemicals and sources of heat, such as sitting in saunas or the sun.
Management of PPES consists of keratolytic agents such as urea ≥ 10% for grade ≥ 1 PPES, with addition of high-potency topical steroids such as fluocinonide 0.05% for grade ≥ 2 symptoms.
Stomatitis / Mouth Sore
Preventive strategies include undertaking dental work aimed at eliminating existing tooth and gum disease before the start of treatment and education regarding the importance of thorough and frequent cleaning of the oral cavity. Avoidance of salty, spicy, or citrus-based foods, as well as hot beverages, may help prevent stomatitis.
Upon emergence of grade 1 or 2 stomatitis, dexamethasone 0.5 mg/5 mL elixir is recommended; an augmented betamethasone dipropionate 0.05% gel applied to gauze and held against the affected surface may also assist in alleviating symptoms.
Also this site gives more suggestions
best
-
joea73
MemberJune 21, 2024 at 7:11 pm in reply to: BCG vs Mitomycin due to Psoriasis treatment with Skyrizi Hello Is it looks likeWhat is happening in our immune system is so complex. I think the medical community knows more about interactions of different immune cells to cause psoriasis than they know about cancer cells are killed by immune responses by introducing BCG bacteria into bladder. The heavy weight immune cells which will bladder cancer cells are Killer T-cells (CD8+). To produce millions of Killer T-cells which knows which cells to attack, Helper T-cells (CD4+) are involved. Helper T-cells much get information about specific cancer cells from antigen presentation cells (APC) such as Dendritic cells and Macrophages. In addition to presenting cancer specific antigens, Dendritic cells and Macrophages secrete various cytokines (like hormones) which act as signal among different immune cells. One of cytokines which Dendritic cells and Macrophages is Interleukin-23. Skyrizi for psoriasis treatment is interleukin-23 inhibitors. I dot not know how interleukin-23 affect T-cell responses by BCG treatment and how much it affects the efficacy of BCG treatment when interleukin-23 are inhibited by Skyrizi. I have not located a clinical trial which tested the effect of BCG treatment while patients are on Skyrizi. But, it makes sense that not to use BCG treatment.
In terms of MMC vs BCG, I have thought BCG is better in recurrence free survival rate and progression free survival rate. But a recent study, by looking at multiple clinical studies on BCG and MMC, came to a conclusion that BCG and MMC are comparable both in recurrence free and progression free survival for Ta and T1 papillary urothelial carcinoma.
-
There was a publication of the study (2021) by MD Andersons about the timing of intravesical BCG and its affects on the effective of the BCG treatment. The conclusion is that the delay does not affect efficacy and side effects. BCG treatment received adequate BCG at a median (range) of 26 (6-188) days from TURBT. Below is the link to the study. So, certain delay in receiving the BCG after TURNT should be okay according to MD Andersons study.
https://pubmed.ncbi.nlm.nih.gov/33783950/
I do not comprehend the pathology result. It sounds like there were high grade papillary tumor(T1HG) and carcinoma in-situ (CIS). At any rate, your NMIBC is considered as high risk.
Before BCG, intravesical chemotherapy was used to treat high risk non muscle invasive bladder cancer (NMIBC))
Back in 2000, the SWOG clinical trial led by Dr. Lamm showed BCG induction ( 6 weekly) and maintenance 3 years reduced recurrence and progression much better than intravesical chemotherapy for high-risk NMIBC.. Intravesical chemotherapy such as MMC can reduce recurrence but not progression as well as BCG.
https://pubmed.ncbi.nlm.nih.gov/10737480/
Incidentally, according to the study (1995) by MD Andersons, von Brunn’s nests itself is not independent risk factor so it should not affect the treatment decision.
-
joea73
MemberJune 6, 2024 at 8:17 am in reply to: Stopping BCG early – implications for tumour recurrenceI have found two studies specifically addressing your question.
One study (Korea) did retrospective study based on published clinical studies. The team split into induction only, one year maintenance, and 3 years maintenance. The study found one year maintenance had less recurrence than induction only, and not much difference between one year and 3 years maintenance in term of recurrence.
The second study (Taiwan) did retrospective study on their own patients (427). The study found patients who had 13-15 BCG treatments had best recurrence free rate. You fit in this 13-15 BCG treatment group.
Recurrence on BCG maintenance duration
Dr. Lamm who had shown induction + 3 year maintenance improve recurrence free and progression survival said that bcg+ 3 year maintenance would reduce recurrence by 27%. If you look at the chart by the Taiwan team, the difference on recurrence is about 30% between the induction vs the induction + maintenance. The study by the Taiwan team and what Dr. Lamm match, indicating the vaidity of the study by the Taiwan team.
-
I think you have already made up your mind, which I think it is correct decision.
First of all, 1/3 dose was chosen, yes as one of strategies to deal with BCG shortage, but because an European study showed reducing to 1/3 dose did not make difference in terms of the efficacy and side effects compared to the full dose. Furthermore, Dr. Ashish Kamat team validated it by comparing randomly 563 patients who received full dose and reduced dosage between 2000 and 2022 at MD Anderson.
BCG dose reduction vs full dose at MD ANDERSONS
Assuming your NIMBC is classified as high risk (T1HG, CIS) for recurrence & progression, 3 year BCG is likely recommend.
You can estimate additional hours of driving by applying # of expected visit to Hopkins.
6 weekly induction and 3 weekly at 3,6,12,18,24,30, 36 months = 27 treatment
I expect cystoscopy & cytology are done a few weeks after each BCG.
Plus CT scan here and thereAfter the completion of three years BCG, follow up by cystoscopy surveillance first couple years -every 3 months, then every 6 months till year 5, then every year life time. Plus CT scan.
If it is low grade, though there may be recurrence, it will be low grade, there is always exceptions, so local hospital should do fine. If it is high grade, it gets tricky such as managing side effects, and dealing when your tumor does not respond to BCG well. Hopkins should have many tools to deal with such situation.
-
Hopkins remind me of 1) 2nd pathology 2) Someone named Greensburg donated $15M which was used for the nation’s only cancer center for bladder cancer – Johns Hopkins Greensburg Bladder Cancer Institute, 3) Dr. Max Cate who is well known in bladder cancer field. Two short videos below can tell what is him like. I often see him in webinars related bladder cancer.
Dr. Max Cates
Dr. Max Cates 2He is doing right now a clinical trial which compares BCG vs Gemcitabine and Docetaxel sequential intravesical chemotherapy.
Because you are 50s young and I am getting closer to 80. Your priority is different from mine. I listened Dr. Cate talking about bladder cancer and one of audience asked about the timing of cystectomy (podcast 10 years ago). I don’t remember exactly, if it is recurrence, T1 with CIS, he would be discussing early cystectomy. He sounds like he wants to dialogue with his patient. I think it would help you finding out a trigger point to consider early cystectomy though I hope you never need to get there.
He is accepting new patients
Dr. Max Cates profileI was never able to establish a relationship of dialogue with my urologist at local hospital. Like you said, I also live 20 mins from the local hospital where it takes 1 hour to a university hospital. I have noticed that my urologist/ hospital not always follow the guidelines. But he also did surgery for my prostate, and I think he is a skilled surgeon. So, I am staying with him, but if any complicated issue happens, I am thinking of getting a second opinion from the university hospit
-
Lymphovascular invasion
Pathologist knows that the importance of identifying Lymphovascular invasion in evaluating tissue sample for NMIBC. If there are such invasion, they will say so. Some pathologist may choose not to say about Lymphovascular invasion if the pathologist does not find it. Mine did not say anything about Lymphovascular invasion. So, I do not think there were any Lymphovascular invasion in the tissue sample. You can always clarify with your urologist because the pathology report is a communication tool between the pathologist and the urologist. FYI, there was a study (2008, Japan) to find out number of lymphatic vessels in the lining of the bladder. The lining of the bladder wall consists of Epithelium(Ta), Lamina propria/connective tissue (T1), Muscularis propria/muscle tissue (T2), serosa, peri vesical fat (T3). We can see that the number of lymphatic vessels in Lamina propria (T1) is much less than in Muscle (T2). I think this is why, once the tumor progresses to the muscle layer of bladder, chance of metastasis increases rapidly, so neoadjuvant chemotherapy to kill circulating cancer cells and RC are commonly recommended to MIBC.
Size/ numbersLocation small Medium Large Epithelium (Ta) 0 0 0 Lamina Propria (T1) 6 4 4.5 Muscularis Propria (T2) 23 17.5 18.5 Serosa (T3) 3 3 `1 Perivesical fat (T3) 2 2.5 4 Thanks for sharing the detail pathology report. It is T1HG non-muscle invasive according to the pathology report.
-
Hello walkslow,
I am also very surprised to hear that the histology (pathology) report came back high grade when cytology was “negative for high grade urothelial carcinoma because usually cytology follows after cystoscopy sees no tumor. At Yale cancer center, of 2570 cytology cases, 0.8% was diagnosed HG when cytology said Negative.
Do you think you can post exact wording of the pathology report? The reason is that your statement of ” it was classified as a high-grade noninvasive urothelial carcinoma (stage T1)” is a bit contradictive. Once tumor goes beyond epithelial issue (Ta or T0) into lamina propria (connective tissue layer), it is T1 and called invasive tumor, but if the tumor has not invaded into the muscle tissue if it called non muscle invasive. We want to clarify it by reading the exact wording of the pathology report.
I think your urologist has done everything what it is supposed be so far. He went ahead order CT scan. He prescribed single chemotherapy wash after the initial TURBT.
Assuming it was indeed T1HG, at this moment, you are likely cancer free. Let me explain it. CT scan showed a single tumor with the size of one inch (less than 3 cm). It means that your urologist should have been able resect the tumor and surrounding residues completely.
Incidentally, if it is T1HG, your urologist is likely recommend the 2nd TURBT. The second TURBT will resect deeper into muscle tissue to make sure the tumor has not progressed to the muscle tissue and may be wider to remove possible residues remained.The single instillation of Gemcitabine is to kill off fragments from the tumor which could have landed on to other parts in bladder, which would reduce the risk of recurrence.
In terms of grading system, we are now using LG and HG, but it used to be G1 (low grade), G2 (intermediate Grade), G3 (high grade).
In Europe, they continued to use G1,2,3 system in addition to LG and HG. According to the recent international society of pathology and European Association of Urology consensus, they are moving toward LG, G2HG and G3HG three tiers classification. The reason is that they have recognized that all HGs are not the same gnomically and in terms of prognosis, Unfortunately, perhaps for the cost reason, genome analysis is not done routinely, so all HGs are being treated the same today. Incidentally G3HG has higher risk of invading into the muscle tissue but G2HG has less risk.Incidentally, I was listening to the old (10 years old) BCAN webinar and a patient asked a question of early cystectomy. The urologist said if there are recurrences of multiple T1 and with CIS, then may recommend cystectomy. Also, the data which showed early cystectomy gives better survival compared to cystectomy after the intravesical treatment failed are retrospective study and has not really proven the case.
Because Negative for HGUC cytology and HG pathology is less than 1% according to Yale Cancer Center stats, perhaps you may want to discuss with your urologist if your tissue sample be re-evaluated by Johns Hopkins. I am not sure it is covered by insurance, but their website says $400 and the website says once they received the slides with tissue sample, you will get the report 48 hours after.
-
Hi Shepman,
Until recently, there were no drug/treatment available for those tumors which did not respond to BCG treatment. There was one FDA approved drug Valrubicin, but it was approve over 20 years ago and efficacy was not so good, so I do not think it is being offered. Often single chemotherapy drug such as mitomycin, gemcitabine was used for BCG unresponsive. But now there are four FDA drugs are available for BCG unresponsive, and several drug/treatment are in later phase of clinical trial.
Pembrolizumab (Keytruda) alone Checkpoint Inhibitor Intravenous FDA approved
Gemcitabine+Docetaxel Existing drugs Intravesical Did not require FDA approval
Nadofaragene (Adstiladrin) Gene Therapy Secreting IFN Intravesical FDA approved
Anctiva + BCG IL15 Superagonist +BCG Intravesical FDA approved
Still on clinical trial
TLD-1433 Photodynamic Therapy Intravesical+Laser Phase 2B
TAR-200 Device to secrete chemo Intravesical Phase 2
Cretostimogene Oncolytic Immunotherapy Intravesical Phase 3
Cretosmitogene + Pembro Oncolytic Immunotherapy Intravesical/Intravenous Phase 2Pembrolizumab +BCG BCG+ immunotherapy Intravesical/Intravenous Phase 3
-
To answer your question, there was a large joint clinical study by MD Andersons Cancer Center in Texas, Moffitt Cancer Center in Florida and Levine Cancer Institute in North Carolina to find out how the timing of BCG after TURBT will affects effective ness of BCG treatment.
Over 500 patients were involved, with a median (range) of 26 (6-188) days from TURBT, their studies showed the following conclusion.
The rates of tolerability and response to adequate BCG are not predicated by the timing of induction BCG instillation after TURBT. Early administration in properly selected patients is safe and delays do not affect therapeutic response. So, I would not worry much yet.
The study on timing of BCG after TURBT
https://pubmed.ncbi.nlm.nih.gov/33783950/As Alan mentioned, if the delay persists without knowing when you have have BCG treatment, one option is to participate on the clinical trial on the clinical trial BRIDGE which is to compare Gemcitabine + Docetaxel intravesical chemotherapy vs BCG for BCG naïve patients.
Gemcitabine + Docetaxel protocol was developed by University of Iowa team under Dr. Michael O’Donnell, who is known as one of early Guru for non muscle bladder cancer along with Dr. Donald Lamm of University of Arizona, now retired. Gemcitabine + Docetaxel protocol was used for those patient who did not respond to BCG, but during BCG shortage, it was used also BCG naïve patients with very good result. I think this trial is good trial for patients because patient will receive either GEM/ODC treatment or BCG treatment.Link to the clinical trial information
https://www.cancer.gov/research/participate/clinical-trials-search/v?id=NCI-2022-04864&r=1best
-
joea73
MemberMarch 6, 2024 at 6:34 pm in reply to: Metastatic Cancer in lymph nodes and Tumor in kidneyThe Padcev with Keytruda was just approved by FDA in December, 2023, but the clinical trial had shown an excellent result such that
55% reduction in the risk of progression compared with chemotherapy, which is somewhat unprecedented. But more importantly, the result also showed an over 50% reduction in the risk of death. In terms of side effects, typical side effects by PADCEV and immunotherapy are expected but the hospital should be able address the side effects as the hospital should have sufficient knowledge in dealing with those side effects by dealing with PADCEV and KEYTRUDA independently. You should be able get the information from the hospital or the oncologist. -
joea73
MemberMarch 6, 2024 at 4:10 pm in reply to: 2nd cytology saying “Negative for HGUC” but raising a problem of LGUN“Negative for HGUC” is the expression used in the new cytology reporting system – The Paris Reporting System for Reporting Cytology (TPS), incorporated around 2015, now 2022 version is TPS 2.0. TPS was developed by American Society of Cytopathologist and International Congress of Cytopathologist. Most cytology lab should have adopted the TPS guidelines. So, the cytology lab who analyzed your urine sample seems to be following the TPO guidelines.
The major shift in its goal is to improve the accuracy by reducing number of Atypical, and in reporting for HGUC only. The rationale for reporting HGUC only is because HGUC can be life threatening if not identified accurately and LGUC is considered non life threatening. Also, gnomically LGUC and HGUC are considered different cancers such that high percentage of LGUC has mutation in FGFR, whereas HGUC shows mutations similar found in muscle invasive bladder cancer.
In term of LGUN or LG Urothelial Neoplasm, I get confused with possible difference between neoplasm and carcinoma, or neoplasm and neoplasia as I have read that they are sometimes used interchangeably though there may be fine differences which I do not know.
In terms of Low Grade urothelial neoplasia, Dr. Adebowale Adeniran, Professor of Pathology and Director of Cytopathology and Cytology Lab at Yale School of Medicine mentioned as follows in his 2020 webinar on TPS.
Low-Grade urothelial neoplasia
Combined cytologic term for low grade papillary urothelial neoplasms which include
Urothelial papilloma, PUNLMP, LGPUC, flat low grade intraurothelial neoplasia
3-dimentional cellular papillary clusters with fibrovascular cores with capillaries
Features
Almost impossible to diagnose without mini-biopsy with fibrovascular core
Cytologically normal nuclei
Is it truly a carcinoma?
More common than HGUC
But NOT life threateningThe thing is that the urologist could not find anything in cystoscopy, CT scan did not find anything. So, the urologist would not know where to get mini biopsy from unless the urologists’ gets it from random locations in bladder.
-
joea73
MemberFebruary 25, 2024 at 1:02 am in reply to: Oncolytic Viruses for the Treatment of Bladder CancerThe phase 3 BOND-003 study (NCT04452591) evaluating cretostimogene grenadenorepvec (formerly, CG0070) had completed enrollment of patients with high-risk non-muscle invasive bladder cancer (NMIBC) unresponsive to Bacillus Calmette-Guerin (BCG). Subsequently, the result of the phase 3 BOND-003 study was announced during Society of Urologic Oncology Annual Meeting (SUOA) in December 2023. The result of the phase 3 showed very good efficacy with little side effects which led to receiving FDA Fast Track Designation for the treatment of patients with BCG-unresponsive CIS with or without Ta/T1 papillary disease.
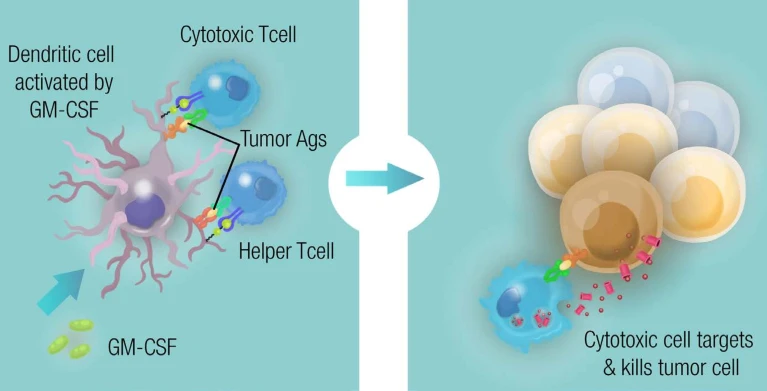
Cretostimogene grenadenorepvec (CG007) belongs to oncolytic virus technology as bellasmith posted. Oncolytic virus uses virus such as common cold virus but edit virus DNA or RNA and remove the gene which causes sickness, then edit DNA or RNA to so the virus achieves intended behavior. In case of CG007, the DNA of the virus was modified so the virus enters into every cell but it only replicate itself in the cell that has an Rb deficiency or defect which is often found in bladder cancer cell. This will ensure only bladder cancer cells will be be affected by CG0070 but not normal cells. In addition, CG0070 encodes the cDNA for human granulocyte macrophage-colony stimulating factor (GM-CSF), a cytokine known to be a potent inducer of specific, long-lasting antitumor immunity in animal model.
In short, CG0070 kills bladder cancer cells in two ways. One is by CG0070 (the virus) replicating in bladder cancer cell and bursting the cancer cell. The other is by the DNA of CG0070 enabling producing human granulocyte macrophage-colony stimulating factor (GM-CSF), which invokes dendritic cell, which then delivers antigen ( information) of bladder cancer to near by lymph nodes, which then produces the tumor specific T-cells which will kill bladder cancer cell. Because CG0070 invokes immune response and those immune cells kill bladder cancer cell, CG0070 is also called oncolytic immunotherapy. CG0070 is considered to give durability response because it invokes T-cells. The efficacy of CG0070 exceeded the efficacy of pembrolizumab (Keytruda) immunotherapy alone for BCG Unresponsive.
Also CG0070 and Pembrolizumab (Keytruda) combination has shown better efficacy than CG0070 alone CORE-1 phase 2 clinical trial.
The summary of efficacy of CG0070 and CG0070 + Pembrolizumab(Keytruda) immunotherapy
BOND-003 CG0070 alone Phase 3
CR at 6 months 44% and at 12 months 28% CG0070 aloneCORE-001 CG0070 + Pembrolizumab (Keytruda) combination Phase 2
Complete Repose Rate 82% at 6 months, 81% at 9 months and 68% 12 months.Mechanism of Action of CG0070
https://www.cancernetwork.com/view/cretostimogene-grenadenorepvec-yields-durable-responses-in-nmibc
-
I only can support you by providing the actual data.
50% of people diagnosed with bladder cancers are TaLG. It is a type of tumor which does not progress. Usually, no further treatment is required after removing tumor (TURBT).
25% are diagnosed with T1HG or CIS which are considered high risk but not invaded to muscle of bladder. Usually treated with BCG into bladder.
20% are diagnosed with T2 and deeper, which invaded muscle of bladder. Typically removal of bladder is recommended because there will be high change that cancer cells migrate to other key organs (metastasis) though blood and lymphatic channels of muscle. If the tumor invaded shallow in to the muscle, they may treat it with Tri-Modal Therapy, which is resect tumor area as much as possible, followed by chemotherapy and radiation. The effectiveness of TMT has shown to be the same as removal of the bladder in selected patients.5% are diagnosed with metastasis.
In case of your data, who is 87 with comorbidity, the hospital may recommend to opt to other treatment than removal of bladder, which used to be typically chemotherapy and radiation. Chemotherapy usually involves cisplatin which is known to work well for bladder cancers but it is known to have side effects – renal toxicity and ototoxicity. Recently, a new treatment was approved. It is a targeted chemotherapy chemotherapy (PADCEV) and immunotherapy combination (Keytruda) which double the survival rate compared to chemotherapy for advanced and metastatic bladder cancer. PADCEV+Keytruda have its own side effect but less than and different from cisplatin based chemotherapy.
I think there are now several options in choosing optimum treatment for your dad depending upon the result of analysis of cancer tissues which will be obtained at TURBT.
Best wishes